Comprehensive biomarker testing is recommended for people with non-small cell lung cancer (NSCLC) because of the many treatment options for known biomarkers—also called driver mutations. People with small cell lung cancer (SCLC) do not need to undergo this testing because there are currently no FDA-approved treatment options for SCLC biomarkers.


We envision a future where there’s No One Missed when it comes to comprehensive biomarker testing. Learn more about how testing could help you find the right lung cancer treatment plan. Explore resources at No One Missed.
Comprehensive biomarker testing is used among diagnosed lung cancer patients to determine the presence of particular mutations or of a particular protein. It is the first step in precision medicine—ensuring that a patient gets matched to the right treatment at the right time, based on the patient's biomarkerA biological molecule found in blood, other body fluids, or tissues that is a sign of a normal or abnormal process, or of a condition or disease. A biomarker can be a change in DNA (mutation), RNA, or protein status.
This section will help patients:
- Understand what a biomarker is
- Learn how biomarkers are used to make lung cancer treatment decisions
- Understand how biomarker testing is done
To help you understand and share this information, you can download our free booklet that summarizes the detailed information here.
For more information on the treatments that may result from biomarker testing, go to Targeted Therapy and Immunotherapy. If your lung cancer is found to be positive for a biomarker, you can find information tailored specifically to your type of cancer on our Patient Gateways.
For a handy biomarker testing reference, download a flyer and share it with your family and healthcare providers.
What is a biomarker?
A biomarker is any molecule that can be measured in tissues, blood, or other bodily fluids. The presence of a biomarker may be a sign of an abnormal bodily process or condition or a disease. A biomarker may also be called a molecular marker, genotype, or signature molecule.1
Biomarkers can be used to:
- Determine whether a disease or condition is present
- Determine how aggressive the disease is
- Predict how well the body will respond to a treatment for a disease or condition
What is biomarker testing? Why is it important to lung cancer patients?
Biomarker testing (also known as mutation, genomic, or molecular testing) is a way for the healthcare team to gather as much information as possible about a patient's unique lung cancer, ideally before treatment begins. It uncovers whether the patient has a treatable driver mutation and establishes the patient's PD-L1Part of the immune system mechanism that keeps T cells from functioning proteinA molecule made up of amino acids that is needed for the body to function properly. Proteins are the basis of body structures, such as skin and hair, and of other substances such as enzymes, cytokines, and antibodies expression level. The results of these tests help determine whether any of the US Food and Drug Administration (FDA)-approved lung cancer targeted therapies or a particular immunotherapy drug is right as part of the patient's treatment plan. Biomarker testing is most often used to plan these treatments for advanced-stage non-small cell lung cancers. (Note that biomarker testing may also be useful in some situations for early-stage lung cancers.2)
What types of biomarkers are used to determine the best treatment for lung cancer patients?
Two types of biomarkers are currently used to help optimize a lung cancer patient's treatment plan: driver mutations within the cancer's DNAThe molecules inside cells that carry genetic information and pass it from one generation to the next. Also called deoxyribonucleic acid to determine whether a targeted therapy might be appropriate and the level of expression of a particular protein, PD-L1, in the patient's tumor to determine whether an immunotherapy drug might be appropriate.
Driver Mutations
All the organs and tissues in our bodies are made up of cells, and each of these cells contains thousands of genesCoded instructions within a cell that control how the cell grows in a systematic and precise way. Genes are made up of DNA, material that carries a specific code that is used to ultimately make proteins that have specific functions for the cell. It is essential for each gene to have the correct DNA code, or instructions, for making its protein. When the DNA is correct, the protein is able to perform the correct function.3
When a gene has an error in its DNA, it is said to be mutated, or changed. Mutations can be:3
- Acquired (or somatic): Present only in the tumor and not passed on to children
- Inherited (or germline): Present in all cells of the body and passed on to children
Virtually all of the biomarkers that are helpful to making treatment decisions in lung cancer are acquired. Inherited biomarkers are still being researched. In this section, we are discussing only acquired mutations.
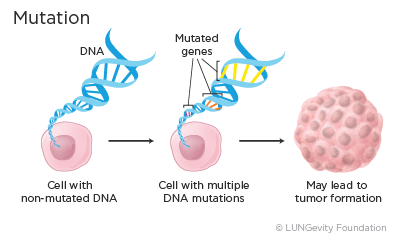
Mutations occur often, and normally the body can correct them. However, depending on where in a gene the change occurs, the small change may go undetected by the body and become part of the cell's blueprint. Over time, an accumulation of mutations can result in the formation of a tumor. Mutations that cause cancer are called driver mutations.3
Several types of driver mutations cause cancer. Some of these are:
- Activating mutation: An activating mutation is a change in the DNA sequence that can cause changes in the protein made by the gene so that the protein is always active, leading to uncontrolled cell growth.4
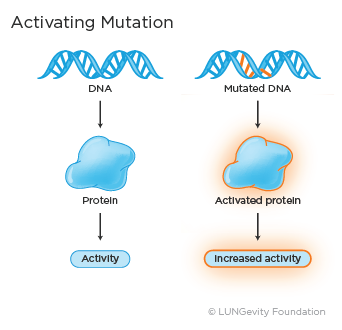
An example of an activating mutation in lung adenocarcinomaA type of non-small cell lung cancer that usually develops in the cells lining the lungs. It is the most common type of lung cancer seen in non-smokers, a type of non-small cell lung cancer (NSCLC), is BRAF V600E.5
- Fusion: Fusion, or rearrangement, occurs when a part of one gene fuses with, or attaches to, a part of another gene. The fused gene then produces a unique protein that promotes abnormal, uncontrolled cell growth.4 The gene rearrangement may also be referred to as a translocation.
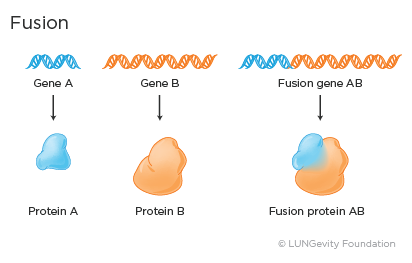
Examples of fusion genes in lung adenocarcinoma include EML4-ALK and CD74-ROS1.6,7
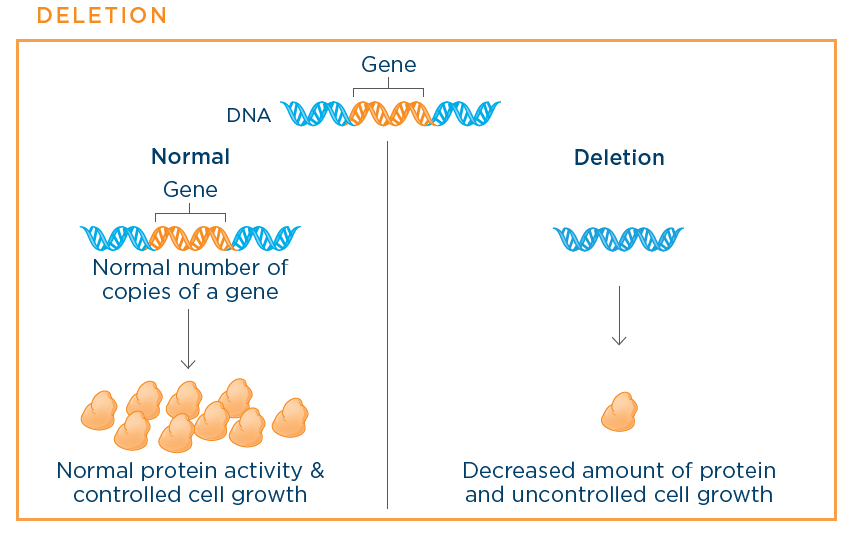
- Amplification: Amplification means that there are many more copies of a gene than normal. This causes overexpression and leads to increased protein activity and uncontrolled cell growth.4
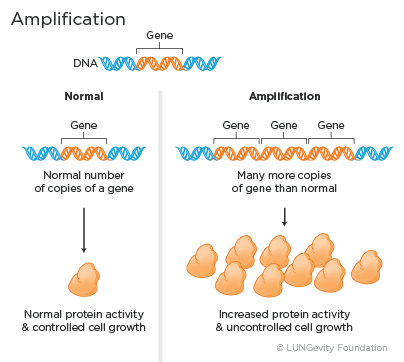
Examples of amplified genes in lung adenocarcinoma include HER2 (ERBB2) and MET.8
- Deletion: Deletion means part of or the entire gene is missing in the cancer cells. The deletion then leads to reduced levels of normal protein being produced by the cancer cell and uncontrolled cell growth.4
Examples of deleted genes in small cell lung cancer (SCLC)A fast-growing cancer that forms in tissues of the lung and can spread to other parts of the body. Named "small" for how the cancer cells look under a microscope include TP53 and RB1.9
A person's lung cancer may or may not have one of the many known driver mutations. So far, scientists have identified more than 20 different driver mutations sometimes found in NSCLC and SCLC, and they are continuing to look for more.9
These driver mutations are biomarkers that are used in biomarker testing in lung cancer; their presence may determine whether a patient will be prescribed one of several approved targeted therapies or be potentially eligible for a clinical trial for a targeted therapy in development.
Right now, scientists have the most information about driver mutations in the subtype of NSCLC called lung adenocarcinoma. In patients with metastatic lung adenocarcinoma, the driver mutations in lung adenocarcinoma that currently have FDA-approved targeted therapy drugs available are ALK, BRAF V600E, EGFR, KRAS G12C, MET exon 14 skipping, NTRK, RET, and ROS1.10
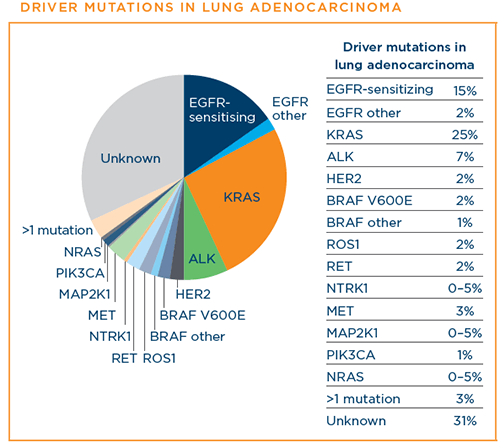
Image source: Hirsch F, et al. New and emerging targeted treatments in advanced non-small-cell lung cancer. Lancet. Vol 388. September 3, 2016
As science progresses, we are also learning about mutations in early-stage lung adenocarcinoma.11
Scientists are also making progress in understanding mutations in squamous cell lung cancer. While driver mutations unique to squamous cell lung cancer have not yet been identified, driver mutations that more commonly occur in lung adenocarcinoma can also occur in squamous cell lung cancer. These include EGFR mutations and MET exon 14 skipping mutations.10,12,13
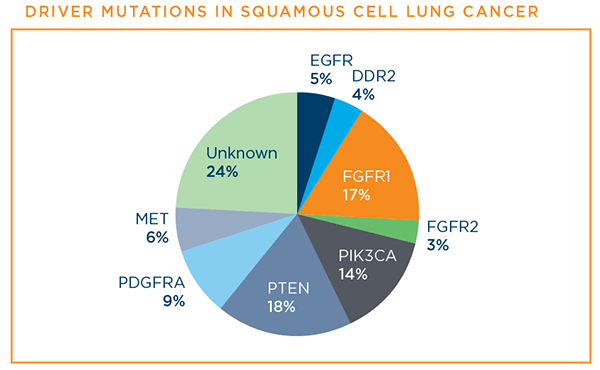
Image source: Hirsch F, et al. New and emerging targeted treatments in advanced non-small-cell lung cancer. Lancet. Vol 388. September 3, 2016.
Driver mutations in SCLC and other types of lung cancer are also being studied. There are as yet no targeted therapies that are FDA-approved for them.14
Immunotherapy Biomarkers
There are several immunotherapy biomarkers; only one, programmed death-ligand 1 (PD-L1) protein, is currently used in the clinic for lung cancer.
Programmed death-ligand 1 (PD-L1) protein
T cells are the major immune cells the body uses to recognize and destroy abnormal cells. However, the immune systemA complex network of cells, tissues, organs, and the substances they make that help the body fight infections and other diseases has fail-safe mechanisms that are designed to control the immune response at appropriate times in order to reduce damage to healthy tissue. These mechanisms are called immune checkpoint pathways. They are essentially the brakes on the immune system. The PD1/PD-L1 proteins are an example of an immune checkpoint pathway. The PD-1 protein is found on T cells and acts as the brakes that keep the T cells from attacking healthy cells. PD-L1 is a protein that is overexpressed on cancer cells. When the PD-1 on T cells attaches to the PD-L1 on cancer cells, the T cells know not to attack the cancer cells. Cancer cells can thus evade detection by T cells, with the result that the T cells' immune response is lessened at a time when it should be active.15
Instead of attacking a patient's cancer cells directly, as targeted therapies do, immunotherapy drugs strengthen the natural ability of the patient's immune system to fight cancer. The type of immunotherapy known as immune checkpoint inhibitorsThe agents that target the pathways that tumor cells use to evade recognition and destruction by the immune system works by targeting and blocking the PD-L1 fail-safe mechanisms of the immune system, allowing the immune system to work better.15
Patients who have a high level of PD-L1 expression are more likely to respond to immune checkpoint inhibitors. However, even those with tumors that express a low level or do not express PD-L1 may respond to these treatments.16
Other immunotherapy biomarkers
There are other types of immunotherapy biomarkers currently being studied, including:1,17,18,19
- Tumor mutational burden (TMB): The total number of mutations (changes) found in the DNA of cancer cells
- CTLA-4: a protein that, when blocked, enhances the immune system's ability to kill cancer cells
- Microsatellite instability: A number of mutations in the microsatellites, which are short, repeated sequences of DNA
When is biomarker testing appropriate?
Biomarker testing may be appropriate:
- When the doctors suspect lung cancer and have recommended a biopsy
- When a patient is already diagnosed with lung cancer
- When a patient's lung cancer recurs (comes back) after treatment
All patients with a lung cancer diagnosis should discuss biomarker testing with their healthcare team.
To find out whether a targeted therapy or immunotherapy may be a good therapeutic option for a patient who has been diagnosed with lung cancer, that patient's tumor tissue or blood can be tested for the presence of driver mutations. The tumor tissue can also be tested for the PD-L1 protein.
Biomarker testing should be an ongoing part of the discussion with a patient's healthcare team. Any decision to test for biomarkers should be made together, and will depend on a number of factors, including the patient's type and stageThe extent of cancer in the body of lung cancer, current treatment plan, overall health, and preferences.
The discussion guide below can help you talk with your doctor about biomarker testing. Click on the picture to get a full-size version you can save or print. It includes a second page where you can take notes when you speak with your doctor.
For which biomarkers should a patient be tested?
Guidelines commonly recommend that all patients diagnosed with advanced-stage lung adenocarcinoma be tested for the ALK, BRAF V600E, EGFR, KRAS, MET exon 14 skipping, NTRK, RET, and ROS1 mutations and the PD-L1 protein. Patients with stage 1B-IIIA NSCLC may consider testing for mutations in the EGFR gene after their tumor has been surgically removed.20
When discussing biomarker testing with the healthcare team, a patient may also want to consider that driver mutations other than ALK, BRAF V600E, EGFR, KRAS, MET exon 14 skipping, NTRK, RET, and ROS1 have been found in both lung adenocarcinoma and squamous cell lung cancers. Drugs that target many of these mutations are being tested through clinical trials, so it is important for patients with NSCLC to consider comprehensive biomarker testing that includes many mutations, rather than just the eight mutations listed above. Patients may also ask about being tested for PD-L1 expression.
If a patient has SCLC, the healthcare team may test for the expression of PD-L1 and small cell-specific biomarkers, such as DLL3, to determine if the patient is eligible for certain clinical trials.
The table below displays common recommendations for biomarker testing. Again, any decision about biomarker testing should be made together by the patient and the healthcare team.21,22,23
|
Type of Lung Cancer |
Stage of Lung Cancer |
Recommendations for Biomarker Testing |
|
Lung adenocarcinoma |
Stages I, II, and III |
Testing for mutations in the EGFR gene should be conducted. Testing for the ALK, BRAF V600E, KRAS, MET exon 14 skipping, NTRK, RET, and ROS1 mutations and PD-L1 protein levels at the time of diagnosis and surgical resection is not always recommended but may be considered. The decision should be made on an individual basis with your doctors. |
|
Stage IV lung adenocarcinoma or lung adenocarcinoma that has recurred or progressed after an initial diagnosis of stage I, II, or III lung cancer in patients who were not previously tested |
Tumors should be tested for ALK, BRAF V600E, EGFR, KRAS, MET exon 14 skipping, NTRK, RET, and ROS1 at the time of diagnosis. Testing for other biomarkers, such as MET amplifications and HER2 (ERBB2) mutations, may be helpful in deciding eligibility for clinical trials. PD-L1 immunohistochemistryA laboratory method that uses antibodies to check for certain antigens (markers) in a sample of tissue. The antibodies are usually linked to an enzyme or a fluorescent dye. After the antibodies bind to the antigen in the tissue sample, the enzyme or dye is activated, and the antigen can then be seen under a microscope. Immunohistochemistry is used to help diagnose diseases, such as cancer. It may also be used to help tell the difference between different types of cancer. is recommended to determine whether you will benefit from an immunotherapy drug in the first-line (initial treatment) setting. |
|
|
Squamous cell lung cancer |
Stages I, II, and III |
Currently, biomarker testing is performed only for clinical trials. |
|
Stage IV |
Consider testing for ALK, BRAF V600E, EGFR, KRAS, MET exon 14 skipping, NTRK, RET, and ROS1 at the time of diagnosis. Testing for other biomarkers, such as MET amplifications and HER2 (ERBB2) mutations may be helpful in deciding eligibility for clinical trials. PD-L1 immunohistochemistry is recommended to determine whether you might benefit from immunotherapy in the first-line setting |
|
|
Small cell lung cancer |
All stages |
Currently, biomarker testing is performed only for clinical trials. |
How is biomarker testing performed?
Currently, tissue biopsies are the only way to confirm a diagnosis of lung cancer; they are also the standard way to detect driver mutations. However, under certain circumstances, your healthcare team may also make use of liquid biopsies, tests done on a sample of blood.
Tissue Biopsies
There are many different biopsy techniques that can be used to obtain the tumor tissue. The technique is determined by the location and size of the tumor, as well as the patient's overall health. The patient's healthcare team will discuss the best options with the patient as well as the risks and benefits of the procedures.
Among the tissue collection techniques are bronchoscopyA procedure that uses a bronchoscope to examine the inside of the trachea, bronchi, and lungs. A bronchoscope is a thin, tube-like instrument wit a light and a lens for viewing. It may also have a tool to remove tissue; this tissue can then be checked under a microscope for signs of disease. The bronchoscope is inserted through the nose or mouth, endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA)A procedure in which bronchoscope fitted with an ultrasound device is guided down the trachea; once in place a needle is inserted through the bronchus and into a lymph node to obtain a sample. EBUS-TBNA requires local anesthesia, transthoracic needle biopsyA procedure in which an interventional radiologist inserts a needle into the chest wall to remove fluid or tissue, thoracoscopyA procedure in which a surgeon makes a small incision in the skin of the chest wall and inserts a special instrument with a small video camera on the end to examine the inside of the chest. Samples of tissue are removed for a pathologist to look at under the microscope. Also called VATS, thoracentesisRemoval of fluid from around the lungs through a hollow needle inserted between the ribs, mediastinoscopyA procedure performed under general anesthesia to get a look at the area between the lungs, or mediastinum. A small incision is made above the breastbone, and a thin tube with a lens for viewing and a tool to remove tissue is inserted. The samples are sent to the lab to check for cancer cells, and mediastinotomyA procedure to get tissue from the area between the lungs. An incision, a little larger than that in a mediastinoscopy, is made near the breast bone and between the left second and third ribs in order to reach lymph nodes unreachable by mediastinoscopy..
Regardless of how the tissue is collected, a patient should confirm with the doctors, before the tissue is removed, that adequate tissue will be collected so that all necessary biomarker tests can be performed. Tissue from the tumor is saved for a long time, so that additional testing, if necessary, can be done. For more details about each biopsy technique, go to Biopsies.
Biomarker testing can be done on both primary tumorsThe original, or first, tumor in the body and metastatic tumors. If the tumor sample is too small to run through multiple tests, priority should be given to testing for mutations that are the most likely to be present, have an FDA-approved drug treatment, or otherwise help with treatment decisions. Therefore, at this time, if there is only a limited amount of tumor tissue, tumors should be tested for the ALK, BRAF V600E, EGFR, KRAS, MET exon 14 skipping, NTRK, RET, and ROS1 mutations.
After the tumor tissue is collected, it is sent to a laboratory for testing. Ideally, comprehensive biomarker testing will be done. In comprehensive biomarker testing, driver mutations in multiple genes are tested for at the same time, rather than sequentially, including not only the ones with approved treatments, but also other known driver mutations. Some of the driver mutations currently without approved treatments may have treatments being tested now or in the near future in clinical trials to which a patient could be matched. An advantage of comprehensive biomarker testing is that when a new mutation target is discovered, it can easily be added to the set of mutations being tested for. Comprehensive biomarker testing is done via a process known as next-generation sequencing, or NGS.
Biomarker testing results are analyzed by a pathologist. All biomarker laboratory results are recorded in a biomarker testing report. It is a good idea to get a copy of your biomarker testing report for your own information and to have it available to show other doctors, if necessary. The test results can take up to four weeks or so to be received by your doctor.24
Liquid Biopsies
Currently, tissue biopsies are the only way to confirm a diagnosis of lung cancer. However, your healthcare team may also use a liquid biopsy instead of a tissue biopsy to decide if certain targeted therapies are right for you.
Liquid biopsies for the detection of driver mutations in lung cancer currently work in this way:25
- When cancer cells die, they release DNA. The DNA then enters the bloodstream in the liquid part of the blood (plasma). This is called circulating tumor DNA, or ctDNA.
- A blood sample is drawn from a vein.
- The blood sample is then sent to the laboratory to check for the presence of driver mutations.
Liquid biopsy test results typically come back sooner from the pathologist than tissue biopsy test results. In addition, the same type of comprehensive biomarker testing for multiple driver mutations done on tissue samples can be done on the blood samples. In several studies, it has been shown that liquid biopsies can be very effective in detecting the driver mutations that have targeted therapies to treat them.25,26,27,28,29,30
At this time, liquid biopsies may help a patient's healthcare team:25,,27
- Determine if a targetable mutation is present at the time of diagnosis and decide if targeted therapies are appropriate
- Check if the patient's cancer has become resistant to a targeted therapy and decide the next treatment option
- Follow the patient's response to a particular targeted therapy
If a liquid biopsy test is negative, results from the tissue biopsy are used to make treatment decisions at diagnosis. If a liquid biopsy is negative and the cancer spreads or comes back, a tissue biopsy may be recommended. It is important to note that not all cancer cells shed DNA, so not all patients can be successfully tested via liquid biopsy.
Are multiple biopsies necessary?
Sometimes, an additional biopsy is recommended. This can happen when:
- Not enough tissue was obtained during the initial, diagnostic biopsy31
- A targeted therapy that worked well against the lung cancer has stopped working and the cancer has recurred. Testing the resistant cancer for additional mutations that may have evolved or rare changes in histology is indicated to help adjust the patient's treatment plan32
- New drugs are approved for the treatment of lung cancer from which a patient might possibly benefit. The new drug or treatment might require biomarker testing
Therefore, a patient's healthcare team may recommend additional biopsies (either tissue or liquid) and biomarker testing at several points in the treatment process. The ultimate decision to have another biopsy should be jointly made by the patient and healthcare team.
What information is included in a biomarker testing report?
At the laboratory, the tissue sample collected during the biopsy procedure is tested and analyzed by a pathologistA doctor who identifies diseases by studying cells and tissues under a microscope or with other equipment. Laboratory results from the biopsy are recorded in a report.
The initial report issued by the pathologist, which includes the diagnosis of lung cancer, its histological type, and its stage, is called the pathology report. (In some cases, limited information about the presence or not of several common biomarkers, including most likely EGFR and ALK, may also be included.)
Most often, however, a separate report from a pathologist with information about a more extensive set of biomarker testing results will follow the initial pathology report. This report is typically called a biomarker testing report (but may also be referred to as a molecular testing report or a genomic testing results report). The biomarker testing report is based on the biomarker testing that occurs after the patient's initial diagnosis of lung cancer. The report contains critical information about a patient's cancer. Specifically, the biomarker testing report indicates whether a patient has biomarkers—either driver mutations or a high level of PD-L1 protein expression—that indicate that a patient may respond to a particular targeted therapy or to an immunotherapy drug, either approved or in clinical development.
The biomarker testing report may take up to several more weeks to be processed. Patients should request a copy of the report for their medical records. Sometimes, the report is also available in a patient’s electronic health records, which are accessible through a hospital’s patient portal. The biomarker testing report may be helpful for discussions with the patient’s healthcare team, to pursue a second opinion about the diagnosis and/or the recommended treatment plan, or to pursue a clinical trial. (Note: The tissue samples will also be needed for a second opinion; as mentioned earlier, these are kept for a long time so will be available.)
Based on conversations with several pathologists, below are the top two things to look for in a biomarker testing report:33,34,35
- Biomarker (mutation or PD-L1 status): This information is on the first page. After the name of each mutation tested for, the report indicates whether or not the mutation is present. In some cases, the report may say “no actionable mutation identified” to indicate that testing did not reveal that the patient has a mutation with an FDA-approved targeted therapy. Likewise, the patient's PD-L1 protein expression level can be found here.
- Appropriate drug for biomarker: Typically, next to the location of the biomarker status, the report notes the drug or drugs (if multiple options are available) that may be effective for a patient with this particular mutation
How do the biomarker test results impact treatment?
If an advanced-stage lung cancer patient's tests are positive for the ALK, BRAF V600E, EGFR, MET exon 14 skipping, NTRK, RET, or ROS1 mutation, there are FDA-approved targeted therapies for each that may be prescribed. For details about targeted therapies, go to Targeted Therapy.
In addition, a certain level of the PD-L1 biomarker will help the healthcare team determine whether a patient is likely to benefit from an FDA-approved immunotherapy drug. For details about immunotherapy treatment, go to Immunotherapy.
Questions to ask your healthcare team about biomarker testing
To help you speak with your healthcare team about biomarker testing, download our Biomarker Conversation Starter.
Before getting biomarker testing:
- What are you trying to find with biomarker tests?
- Have I already had any biomarker tests? Which ones?
- Who performs these tests?
- How are the tests performed?
- Are there any complications from these tests?
- How long will it take to get the test results?
- Where can I get more information about biomarker testing?
- Are there any limitations of biomarker testing?
- Will insurance pay for these tests?
After getting biomarker testing:
- What tests were done?
- What are the results of these tests?
- How will the results affect my treatment?
- The test results are negative: should I be retested?
- The test results are not clear: should I be retested?
- Are there any medications that target my type of lung cancer?
- Will I need these tests again? If so, why? When?
- Are there any clinical trials open to me based on these results?
- How can I get a copy of my biomarker testing report?
Updated February 9, 2024
References
- NCI Dictionary of Cancer Terms. https://www.cancer.gov/publications/dictionaries/cancer-terms. Accessed February 5, 2024.
- Lung Cancer: Metastatic—Non-Small Cell Lung Cancer. NCCN Guidelines for Patients. Version 5.2019. https://www.nccn.org/patients/guidelines/content/PDF/lung-metastatic-patient.pdf. Version 3.2023 – April 13, 2023. Accessed February 5, 2024.
- The Genetics of Cancer. Cancer.Net website. https://www.cancer.net/navigating-cancer-care/cancer-basics/genetics/genetics-cancer. Updated November 2022. Accessed February 5, 2024.
- Pao W, Ladany M. Detecting Gene Alterations in Cancers. My Cancer Genome website. https://www.mycancergenome.org/content/page/detecting-gene-alterations-in-cancers. Updated May 27, 2019. Accessed February 5, 2024.
- Auliac JB, Bayle S, Vergnenegre A, et al. Patients with non-small cell lung cancer harboring a BRAF mutation: a multicentre study exploring clinical characteristics, management, and outcomes in a real-life setting: EXPLORE GPPC -2-14. Curr. Oncol. 2018;25(5):e398-e402. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6209546/. Accessed February 5, 2024.
- Solomon B, Lovly C. Anaplastic lymphoma kinase (ALK) fusion oncogene positive non-small cell lung cancer. In: Lilenbaum RC, ed. Uptodate. Waltham, MA; UpToDate, Inc. 2021. https://www.uptodate.com/contents/anaplastic-lymphoma-kinase-alk-fusion-oncogene-positive-non-small-cell-lung-cancer/print. Updated April 3, 2023. Accessed February 5, 2024.
- Li Z, Shen L, Ding D, et al. Efficacy of crizotinib among differen types of ROS1 fusion partners in patients with RO1-rearranged non-small cell lung cancer. J Thorac Oncol. 2018:13(7):987-995. Accessed February 5, 2024.
- Oh D-Y, Jung K, Song J-Y, et al. Precision medicine approaches to lung adenocarcinoma with concomitant MET and HER2 amplification. BMC Cancer. 2017 Aug 10;17(1):535. Accessed February 5, 2024.
- Byers LA, Rudin CM. Small Cell Lung Cancer: Where Do We Go From Here? Cancer. 2015 Mar 1;121(5):664-672. Accessed November 17, 2020. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5497465/. Accessed February 5, 2024.
- Hirsch FR, Suda Km, Wiens J, Bunn PA, Jr. New and emerging targeted treatments in advanced non-small-cell lung cancer. Lancet. Sep 3, 2016; 388(10048): 1012-1024. Accessed February 5, 2024.
- Skoulidis F, Heymach J. Co-occurring genomic alterations in non-small cell lung cancer biology and therapy. Nat Rev Cancer. 2019;19(9)495-509. Accessed February 5, 2024.
- Comprehensive genomic characterization of squamous cell lung cancer. The Cancer Genome Atlas Research Network. Nature. 2012;489:519-525. Accessed February 5, 2024.
- Perez-Moreno P, Brambilla E, Thomas R, Soria J-C. Squamous cell carcinoma of the lung: molecular subtypes and therapeutic opportunities. Clin Cancer Res. 2012;18(9):2443-2451. Accessed February 5, 2024.
- Rudin C, Poirier JT, Byers LA, et al. Molecular subtypes of small cell lung cancer: a synthesis of human and mouse model data. Nat Rev. Cancer. 2019;19(5):289-297. Accessed February 5, 2024.
- Frequently asked questions about Keytruda. "What are PD-1 and PD-L1?" Keytruda website. https://www.keytruda.com/keytruda-faq/#what-are-pd1-and-pdl1. Accessed Accessed February 5, 2024.
- Onoi K, Chihara Y, Unchino J, et al. Immune checkpoint inhibitors for lung cancer treatment: a review. J Clin Med. 2020;9(5):1362. Accessed February 5, 2024.
- Hellman MD, Ciuleanu T-E, Pluzanski A, et al. Nivolumab plus ipilimumab in lung cancer with a high mutational burden. N Eng J Med. 2018;378(22):2093-2104. Accessed February 5, 2024.
- Topalian SL, Taube JM, Andrews RA, Pardoll DM. Mechanism-driven biomarkers to guide immune checkpoint blockade in cancer therapy. Nat Rev Cancer. 2016;16(5);275-287. Accessed February 5, 2024.
- Tumor Mutational burden (TMB). Caris Molecular Intelligence website.https://www.carismolecularintelligence.com/tumor-mutational-burden-tmb/#:~:text=TMB%20is%20a%20Pan%2DTumor%20Biomarker%20for%20IO%20Response&text=The…. Accessed February 5, 2024.
- FDA approves osimertinib as adjuvant therapy for non-small-cell lung cancer with EGFR mutations. U.S. FDA website. https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-osimertinib-adjuvant-therapy-non-small-cell-lung-cancer-egfr-mutations. Posted December 18, 2020. Accessed February 5, 2024.
- Non-Small Cell Lung Cancer (NSCLC)—NCCN Clinical Practices Guidelines in Oncology. https://www.nccn.org/professionals/physician_gls/pdf/nscl.pdf. Version 1.2024 – December 21, 2023. Accessed February 5, 2024.
- Updated Molecular Testing Guideline for the Selection of Lung Cancer Patients for Treatment with Targeted Tyrosine Kinase Inhibitors. Association for Molecular Pathology website. https://www.amp.org/clinical-practice/practice-guidelines/updated-molecular-testing-guideline-for-the-selection-of-lung-cancer-patients-for-treatment…; Posted January 2018. Accessed February 5, 2024.
- Small Cell Lung Cancer (SCLC)—NCCN Clinical Practice Guidelines to Oncology. https://nccn.org/professionals/physician_gls/pdf/sclc.pdf. Version 2.2024 – November 21,2023. Accessed February 5, 2024.
- Reading a pathology report. Cancer.Net website. https://www.cancer.net/navigating-cancer-care/diagnosing-cancer/reports-and-results/reading-pathology-report. Approved March 2019. Accessed February 5, 2024.
- Lovly CM, Berger MF, Vnencak-Jones CL. Circulating DNA. My Cancer Genome website. https://www.mycancergenome.org/content/page/circulating-dna/. Updated April 3, 2019. Accessed February 5, 2024.
- Liquid Biopsy. LabTests Online website. https://labtestsonline.org/tests/liquid-biopsy. Last modified Aug 21, 2021. Accessed February 5, 2024.
- Revelo AE. Martin A, Velasquez R, et al. Liquid biopsy for lung cancers: an update on recent developments. Ann Transl Med. 2019;7(15):349. Accessed February 5, 2024.
- FDA approves first liquid biopsy next-generation sequencing companion diagnostic test. U.S. FDA website. https://www.fda.gov/news-events/press-announcements/fda-approves-first-liquid-biopsy-next-generation-sequencing-companion-diagnostic-test. Posted August 7, 2020. Accessed February 5, 2024.
- Ingram I. Second liquid biopsy ok'd for tumor profiling in all solid cancers. MedPage Today website. https://www.medpagetoday.com/hematologyoncology/prostatecancer/88298. Posted August 27, 2020. Accessed February 5, 2024.
- FDA approves liquid biopsy NGS companion diagnostic test for multiple cancers and biomarkers. U.S. FDA website. https://www.fda.gov/drugs/fda-approves-liquid-biopsy-ngs-companion-diagnostic-test-multiple-cancers-and-biomarkers. Posted November 6, 2020. Accessed February 5, 2024.
- Nassar A. Biopsy: 5 things every patient should know. Cancer.Net website. https://www.cancer.net/blog/2016-05/biopsy-5-things-every-patient-should-know. Posted May 31, 2016. Accessed February 5, 2024.
- Bradley JD. Multiple biopsies may help identify, treat resistance in NSCLC. Healio Hematology/Oncology website. https:/www.healio.com/news/hematology-oncology/20170317/multiple-biopsies-may-help-identify-treat-resistance-in-nsclc. Posted March 17, 2017. Accessed February 5, 2024.
- Interview with Lija Joseph, MD, Lowell General Hospital, Lowell, Massachusetts. July 17, 2019.
- Interview with Timothy Craig Allen, MD, JD, FCAP. University of Mississippi Medical Center, Jackson, Mississippi. July 16, 2019.
- Interview with Tabetha Sundin, PhD, HCLD (ABB), MB (ASCP). Sentara Healhcare, Norfolk, Virginia. June 27, 2019.